Specialty Pharmacy Accreditation: The Complete Guide for 2026

Specialty pharmacy accreditation is often treated like an internal pharmacy checklist: patient management, dispensing, documentation, quality systems, and performance improvement.
Those pieces matter. But they are not the whole operating picture.
For specialty pharmacies, accreditation does not stop at the pharmacy counter. It extends across the full accreditation footprint: pharmacy operations, partner ecosystem, last-mile delivery, and the audit record that proves what happened.
That matters because specialty pharmacy work is increasingly complex. Many therapies require special handling, patient support, payer reporting, REMS coordination, limited distribution participation, or temperature-sensitive delivery. Once a medication leaves the pharmacy, the courier becomes part of the evidence trail.
The question is not only whether the prescription was filled correctly.
It is whether the medication was delivered through the right process, documented clearly, protected during handoff, and traceable if a payer, manufacturer, accreditor, or internal quality team asks for proof later.
This guide explains what specialty pharmacy accreditation is, how ACHC and URAC compare, which requirements matter most, and how last-mile delivery can affect accreditation readiness, especially for pharmacies delivering directly to patients.
What Is Specialty Pharmacy Accreditation?

Specialty pharmacy accreditation is a formal review process that evaluates whether a pharmacy meets recognized standards for safe, consistent, documented specialty medication services.
The commercial risk is not usually one dramatic failure. It is the slow accumulation of small gaps that become hard to defend: a delivery exception with no useful note, a missing signature, a temperature-sensitive shipment with unclear timing, a patient complaint that cannot be matched to a courier record, or a manufacturer inquiry that takes three teams to answer. Accreditation helps pharmacies prove that their operating model can hold up under that kind of scrutiny.
It helps verify that the pharmacy has the systems, policies, workflows, and quality controls needed to support patients taking complex medications. These therapies may require special storage, special handling, clinical monitoring, patient education, adherence support, payer reporting, or additional documentation.
NABP describes its specialty pharmacy accreditation as a three-year accreditation for pharmacies providing advanced pharmacy services and disease management for patients taking medications with special handling, storage, and dispensing requirements. Its review emphasizes patient management, drug quality management, regulatory compliance, quality, and safety through its NABP specialty pharmacy accreditation requirements.
What accreditation verifies
Specialty pharmacy accreditation typically reviews areas such as:
- Patient management
- Clinical support and communication
- Drug procurement and inventory
- Dispensing and distribution
- Quality management
- Regulatory compliance
- Performance improvement
- Documentation and recordkeeping
The exact standards depend on the accrediting body and program scope. But the larger goal is consistent: accreditation helps demonstrate that the pharmacy can manage specialty medication workflows in a safe, documented, repeatable way.
Who specialty pharmacy accreditation is for
Specialty pharmacy accreditation applies to pharmacies that serve patients taking complex, high-cost, high-touch, or clinically sensitive therapies.
That can include independent specialty pharmacies, health-system specialty pharmacies, mail-order pharmacies, pharmacy chains, and other organizations that meet accreditor eligibility criteria. These pharmacies may support medications used for rare diseases, chronic conditions, oncology, inflammatory diseases, gene therapies, or other complex treatment areas.
Why it matters beyond compliance
Accreditation is not just a certificate for the wall.
It can influence payer network participation, manufacturer confidence, limited distribution drug access, REMS readiness, and overall operational credibility. URAC notes that specialty pharmacies are increasingly in the care management business and that accreditation can demonstrate value to payers, manufacturers, and providers through its URAC specialty pharmacy accreditation standards.
For pharmacy leaders, accreditation is commercial infrastructure. It helps show that the organization can handle specialty medication complexity without relying on informal processes, disconnected documentation, or vendor relationships that cannot support the pharmacy’s quality expectations.
Why Specialty Pharmacy Accreditation Matters Commercially
Specialty pharmacy accreditation matters because the business of specialty pharmacy depends on trust.
Payers need confidence that the pharmacy can support covered patients safely and consistently. Manufacturers need confidence that therapies will be handled correctly and documented appropriately. Health systems and providers need confidence that the pharmacy can support patient access without adding avoidable operational risk.
1. Payer network access
Payer networks often expect specialty pharmacies to demonstrate strong patient management, reporting, quality controls, and operational maturity. Accreditation helps provide an external signal that the pharmacy has documented systems for patient care, communication, dispensing, quality review, and regulatory compliance.
The practical issue is evidence. A payer evaluating network participation does not only care that the pharmacy says it has a process. It wants confidence that the pharmacy can show how that process works across the patient experience.
For direct-to-patient specialty pharmacy delivery, that may include whether the pharmacy can document delivery timing, failed attempts, patient communication, handoff confirmation, and exceptions that could affect therapy start or continuation.
Accreditation alone does not guarantee network access. But without strong accreditation readiness, a specialty pharmacy may face a harder path when trying to prove reliability to payers, PBMs, and other network stakeholders.
2. Manufacturer and limited distribution drug relationships
Manufacturers of specialty therapies need confidence that pharmacy partners can protect product integrity, support patient access, manage documentation, and handle exceptions.
That is especially important for limited distribution drugs. When therapy access depends on a smaller network of approved pharmacies, manufacturers may look closely at whether each pharmacy can support the clinical, operational, and reporting requirements attached to the product.
A weak distribution process, poor documentation, missed patient handoffs, or unclear exception management can create friction in those relationships.
3. REMS readiness
Some specialty medications are subject to Risk Evaluation and Mitigation Strategies. The FDA defines a REMS as a drug safety program that may be required for certain medications with serious safety concerns to help ensure the benefits outweigh the risks. FDA guidance on Risk Evaluation and Mitigation Strategies also notes that REMS are designed to reinforce medication use behaviors and actions that support safe use.
For specialty pharmacies, REMS-related workflows may include documentation, patient communication, enrollment verification, dispensing controls, provider coordination, or other safety steps. Accreditation-ready systems make those requirements easier to manage because the pharmacy is already operating with structured processes and audit-ready records.
4. Enterprise credibility
Specialty drug spend and operational pressure continue to rise. Mercer projects specialty drugs will account for over half of drug spend in 2025-2026 and beyond, with specialty drug trend projections ranging from 6.5% to 10.5% for 2025-2026 in its Medicaid-focused analysis. Specialty drugs account for over half of drug spend is not just a cost headline. It is a signal that specialty pharmacy operations are becoming more important, more scrutinized, and more expensive to get wrong.
Accreditation helps specialty pharmacies show that their operating model can support that pressure. Strong pharmaceutical logistics compliance practices are part of that model, especially when specialty medications move outside the pharmacy and into direct-to-patient delivery.
ACHC vs. URAC Specialty Pharmacy Accreditation
ACHC and URAC are two of the major accrediting bodies specialty pharmacies commonly evaluate. Many pharmacies also consider NABP and other programs depending on business model, payer requirements, manufacturer expectations, and network participation goals.
The right path depends on the pharmacy’s services, stakeholder requirements, and operating footprint. Some organizations pursue one accreditation. Others pursue dual accreditation to satisfy broader payer, manufacturer, and health-system expectations.
What ACHC evaluates
ACHC offers pharmacy accreditation across multiple pharmacy types, including specialty pharmacy, mail order pharmacy, infusion pharmacy, long-term care pharmacy, and compounding-related programs.
ACHC’s pharmacy page is especially useful for understanding why distribution and delivery belong in the accreditation conversation. ACHC states that mail order pharmacies focus on prescription medications delivered by qualified distribution methods directly to consumers, and that standards address pharmacy licensure, shipping methodology, patient and employee safety, prescription intake and review, patient records and communication, personnel training, organizational oversight, and ongoing quality improvement. Its specialty pharmacy description also includes dispensing medications to a patient’s home, physician’s office, or clinic through its ACHC pharmacy accreditation standards for shipping and distribution.
That makes ACHC an important source for this article’s central point: delivery is not just a logistical afterthought. In direct-to-patient specialty pharmacy models, distribution and documentation can sit inside the pharmacy’s accreditation footprint.
What URAC evaluates
URAC’s Specialty Pharmacy Accreditation focuses on quality patient care, care management, clinical services, process improvement, risk management, and stakeholder value.
URAC says specialty pharmacies that demonstrate quality patient care are in demand and that accreditation demonstrates value in delivering enhanced clinical services to payers, manufacturers, and providers. URAC also notes that once an organization begins the process, it can be fully accredited in six months or less.
URAC’s emphasis is especially relevant for pharmacies looking to demonstrate quality, accountability, and market credibility across payer and manufacturer relationships.
Where ACHC and URAC overlap
ACHC and URAC have different structures and language, but they overlap in several practical areas:
| Area | ACHC | URAC | Why it matters |
| Patient management | Reviews patient-focused pharmacy services and communication | Emphasizes care management and quality patient care | Specialty pharmacies need documented patient support, not informal follow-up |
| Medication handling | Covers pharmacy operations, distribution, records, and safety | Supports quality and risk management expectations | Product integrity depends on controlled workflows |
| Documentation | Addresses patient records, communication, training, and oversight | Emphasizes metrics, measures, quality, and process improvement | Survey readiness depends on accessible evidence |
| Distribution relevance | Strong direct language around shipping and qualified distribution methods | Broader quality and accountability lens | Courier records can support both operational and quality expectations |
| Performance improvement | Includes ongoing quality improvement | Includes quality measures, risk management, and process improvement | Delivery failures and exceptions should feed quality review |
For pharmacy leaders, the decision is less about which accreditor is “better” and more about which standard set matches the pharmacy’s operating reality.
A pharmacy with significant direct-to-patient delivery volume should pay close attention to how each accreditation path treats distribution, documentation, quality improvement, and partner oversight. A pharmacy pursuing payer or manufacturer contracts should also consider which accreditations those stakeholders recognize, prefer, or require.
The best accreditation strategy starts with the business model: what therapies the pharmacy dispenses, how patients receive them, which payers and manufacturers matter, and which parts of the workflow depend on outside partners.
Why many specialty pharmacies pursue dual accreditation
Many larger or more complex specialty pharmacies pursue dual accreditation to satisfy different stakeholder expectations. A payer may prefer one accreditor. A manufacturer may recognize another. A health system may want broader evidence of quality, safety, and operational maturity.
Dual accreditation can also help pharmacies build a more complete compliance and quality framework. One program may sharpen internal pharmacy operations. Another may strengthen payer or manufacturer credibility. Together, they can support a broader market access strategy.
That said, dual accreditation should not be pursued as a vanity exercise. It adds operational work, documentation demands, and ongoing maintenance. The practical question is whether the accreditation mix matches the pharmacy’s payer contracts, manufacturer relationships, services, and growth plan.
Specialty Pharmacy Accreditation Requirements and Standards
Specialty pharmacy accreditation requirements vary by accrediting body, but most programs review the pharmacy’s ability to manage complex therapies safely, consistently, and with clear documentation.
The requirements should not be treated as isolated checkboxes. They work together. Patient management depends on communication. Dispensing depends on inventory control. Distribution depends on courier performance. Quality management depends on usable records. Performance improvement depends on data the team can actually retrieve.
1. Patient management
Patient management standards often focus on how the pharmacy supports patients throughout therapy.
That can include:
- Patient onboarding
- Clinical assessment
- Medication counseling
- Adherence support
- Side effect monitoring
- Therapy coordination
- Patient communication
- Escalation pathways
- Documentation of interventions
This is where delivery becomes relevant sooner than many teams expect. A patient can receive excellent counseling and still miss therapy if a delivery attempt fails, a package arrives outside the expected window, or the pharmacy cannot clearly explain what happened.
Missed deliveries, unclear handoffs, poor communication, and weak exception handling can all affect patient experience and continuity of therapy. They may not originate inside the pharmacy, but they still touch the patient.
2. Drug procurement and inventory
Accreditation standards commonly examine how the pharmacy procures, receives, stores, tracks, and protects medications.
For specialty therapies, this can include special handling requirements, inventory controls, storage conditions, lot tracking, expiration monitoring, and temperature-sensitive workflows. NABP’s specialty pharmacy accreditation language specifically references medications that require special handling, storage, and dispensing requirements through its NABP specialty pharmacy accreditation requirements.
The last-mile handoff should not become a gap in that control environment. If a medication is temperature-sensitive, high-value, or clinically urgent, the pharmacy needs a clear process for how it moves from inventory to dispensing to delivery.
That is why cold chain logistics in healthcare should be considered part of the operational conversation, not a separate shipping detail.
3. Dispensing and distribution
Dispensing and distribution are where the pharmacy’s internal work meets the outside world.
This section should be treated as one of the most important parts of accreditation readiness, especially for pharmacies delivering directly to patients.
Relevant controls may include:
- Dispensing accuracy
- Package preparation
- Distribution method
- Secure release to courier
- Patient delivery instructions
- Package condition documentation
- Delivery confirmation
- Failed delivery handling
- Return-to-pharmacy procedures
- Exception documentation
A practical test: choose one recent direct-to-patient specialty medication order and follow the record from dispense to delivery.
Can the team see when the order was packed, when it was released to the courier, who accepted custody, when delivery was attempted, who received it, whether a signature was required, and what happened if the first attempt failed?
If the answer requires screenshots from one system, emails from another, a courier portal login, and a manual note from a dispatcher, the pharmacy may have a documentation problem hiding inside a delivery workflow.
ACHC’s pharmacy accreditation language is useful here because it explicitly connects direct-to-consumer delivery with qualified distribution methods, shipping methodology, records, communication, training, oversight, and quality improvement.
For a specialty pharmacy, “delivered” is rarely enough. Distribution needs to produce evidence: what was sent, when it left, who handled it, where it went, whether the handoff was completed, and what happened if the delivery did not go as planned.
4. Quality management
Quality management turns pharmacy operations into a repeatable, reviewable system.
This can include:
- Written policies and procedures
- Staff training records
- Incident reporting
- Corrective and preventive actions
- Complaint review
- Vendor performance monitoring
- Internal audits
- Exception logs
- Documentation standards
The partner ecosystem belongs here. If courier performance affects patient access, delivery reliability, temperature-sensitive handling, proof of delivery, or documentation quality, it should not sit outside the pharmacy’s quality review process.
For example, if a courier repeatedly misses delivery windows for temperature-sensitive medications, that is not just a transportation issue. It may be a quality management signal. The pharmacy should be able to see whether those misses are isolated, recurring by route, tied to specific delivery windows, connected to packaging constraints, or creating patient complaints.
That is the difference between having a vendor and managing a partner inside the accreditation footprint.
5. Performance improvement
Performance improvement is where the pharmacy shows that it does not merely document problems. It learns from them.
Useful delivery-related inputs may include:
- Failed delivery rates
- Reattempt frequency
- Late delivery trends
- Temperature exception trends
- Missing signature rates
- Patient unavailable patterns
- Delivery documentation gaps
- Courier escalation response times
- Return-to-pharmacy events
These metrics can help pharmacy leaders identify operational friction before it becomes a larger compliance, payer, manufacturer, or patient experience issue.
Standard domains and last-mile implications
| Accreditation domain | What it typically evaluates | Last-mile implication |
| Patient management | Communication, counseling, adherence support, issue escalation | Delivery delays or failed handoffs can affect therapy continuity and patient experience |
| Drug procurement and inventory | Product integrity, storage, special handling, inventory controls | The release from pharmacy to courier must preserve documentation and control |
| Dispensing and distribution | Accurate fulfillment, safe delivery method, delivery confirmation | Courier workflows should support traceable handoff and exception management |
| Quality management | Policies, incident tracking, vendor review, corrective action | Courier performance should be reviewed when it affects delivery outcomes |
| Performance improvement | KPI review, trend analysis, process improvement | Delivery data can identify recurring issues before they become audit problems |
This is the accreditation footprint in practice: pharmacy operations, partner ecosystem, last-mile delivery, and audit record.
What’s in Focus for Specialty Pharmacy Accreditation in 2026?
For 2026, the practical question is not only whether policies exist. It is whether the pharmacy can show how those policies work across the full fulfillment and delivery workflow.
That distinction matters.
Accreditation-ready pharmacies need more than policy binders. They need evidence that daily operations match documented procedures and that exceptions are captured clearly enough to support quality review.
Areas likely to receive continued operational focus include:
- Documentation discipline
- Distribution visibility
- Vendor and partner oversight
- Cold chain documentation
- REMS-related workflow control
- Quality improvement evidence
- Audit trail retrievability
- Delivery exception management
In practice, this means pharmacies should pressure-test the handoffs.
A policy may say temperature-sensitive medications are shipped using approved packaging and delivered through an approved courier. But the operational question is sharper: what happens when the patient is not home, the route is delayed, the package is returned, or the delivery record is incomplete?
Survey readiness depends on whether those moments are anticipated, documented, and reviewed. The weak point is often not the written policy. It is the exception path.
FDB has framed specialty pharmacy accreditation as an ongoing operational challenge, noting that many organizations still rely on manual mapping of standards to documentation systems and that this can create strain and risk as teams scale. Its article on specialty pharmacy accreditation documentation requirements also points to the need to embed accreditation alignment into daily workflows rather than treat it as a reactive audit exercise.
That same logic applies to delivery. If distribution is part of the workflow, then delivery documentation should not live in a separate black box.
Specialty pharmacies should be able to answer:
- Which deliveries failed?
- Which were delayed?
- Which required a signature?
- Which involved temperature-sensitive product?
- Which triggered escalation?
- Which records can be retrieved quickly?
- Which courier trends should feed quality improvement?
For a deeper look at operational risks in this area, see Dropoff’s guide to specialty pharmacy delivery challenges.
How Last-Mile Delivery Affects Specialty Pharmacy Accreditation

Last-mile delivery affects accreditation readiness because it is often the last documented step between the pharmacy and the patient.
When specialty medications move through direct-to-patient delivery, the courier may influence several accreditation-sensitive areas: PHI handling, product integrity, chain of custody, proof of delivery, exception management, and audit record completeness.
The pharmacy owns the accreditation. But delivery partners can affect whether the pharmacy can prove that its distribution process is controlled.
HIPAA, PHI, and BAA coverage
Specialty pharmacy deliveries may involve protected health information or other sensitive patient details. Pharmacy teams should evaluate courier relationships carefully, but they should avoid blanket assumptions.
HHS states that the HIPAA Privacy Rule does not require covered entities to enter into business associate contracts with the U.S. Postal Service, certain private couriers, and similar entities when they act merely as conduits for protected health information and do not access it except on a random or infrequent basis as necessary for transportation. The HHS guidance on couriers and HIPAA business associate status is important because it adds nuance: courier status depends on the role, access, and services involved.
In practice, pharmacies should work with legal and compliance teams to determine whether a courier is acting only as a conduit or performing services that involve PHI access, use, storage, or disclosure.
The point is not to assume every courier relationship requires the same documentation. The point is to evaluate the relationship before survey season, not during it.
For more context, see Dropoff’s guide to HIPAA-compliant medical courier shipping.
Cold chain integrity
Some specialty medications are temperature-sensitive. Even when packaging is prepared correctly, the last mile can still create risk through delays, missed handoffs, long dwell times, failed delivery attempts, or unclear return procedures.
Cold chain readiness should include more than packaging materials. Pharmacy teams should understand:
- How temperature-sensitive deliveries are scheduled
- How delays are escalated
- How failed delivery attempts are documented
- How returns are handled
- How delivery windows are monitored
- Whether records can be retrieved during audit or quality review
The last mile is where “stored properly” has to become “delivered properly,” with enough documentation to show the difference.
Chain of custody
Chain of custody matters when a pharmacy needs to show who handled a medication, when custody changed, where the package went, and what happened during exceptions.
For controlled substances, high-value medications, limited distribution drugs, or other sensitive therapies, vague handoff records can create avoidable risk.
A stronger courier workflow should support:
- Clear pickup records
- Time-stamped handoffs
- Driver identification or courier assignment
- Delivery location confirmation
- Recipient verification when required
- Exception notes
- Return-to-pharmacy documentation when delivery fails
Chain of custody does not need theater. It needs usable records.
Proof of delivery and signature capture
Proof of delivery should support auditability, not just customer service.
A useful proof-of-delivery record may include:
- Delivery time
- Delivery location
- Recipient name or signature when required
- Courier record
- Delivery status
- Exception notes
- Photo or digital confirmation, where appropriate
- Reattempt or return documentation
Pharmacies should also define what proof of delivery is expected for different delivery types. A routine refill, a high-value specialty medication, a temperature-sensitive shipment, and a controlled substance may not require the same level of verification.
The courier workflow should match the medication risk, patient context, and documentation requirement. Otherwise, every delivery is treated the same until one of them needs to be defended.
For specialty pharmacies, proof of delivery can help support patient communication, internal quality review, payer inquiries, manufacturer reporting, and accreditation readiness.
A delivery status that simply says “completed” may not be enough when the pharmacy needs to explain the details later.
Delivery exceptions and audit trails
Every pharmacy has exceptions. The problem is not that exceptions happen. The problem is when exceptions happen and the record is too thin to be useful.
Common delivery exceptions include:
- Failed delivery attempts
- Patient unavailable
- Wrong or incomplete address
- Delivery outside the expected window
- Temperature concern
- Package returned to pharmacy
- Damaged package
- Missing signature
- Delayed route
- Reattempt required
Each exception should leave behind enough information for the pharmacy to understand what happened and improve the process.
That is why courier data should be more than a logistics status feed. It should be part of the pharmacy’s operational evidence.
Tracking vs. Auditability: Why Visibility Alone Is Not Enough
Tracking and auditability are related, but they are not the same.
Tracking answers: where is the delivery right now?
Auditability answers: what happened, who handled it, when did it happen, was the handoff verified, were exceptions documented, and can the pharmacy prove it later?
For a specialty pharmacy, tracking is useful during the delivery. Auditability is useful after the delivery, especially if a patient calls, a payer asks, a manufacturer requests documentation, or an accreditation surveyor reviews the pharmacy’s distribution process.
A delivery tracking page may help operations locate a package in real time. But an audit-ready record needs more structure. It should capture the facts that matter after the moment has passed.
That can include time stamps, courier assignment, pickup and drop-off confirmation, delivery location, signature capture, exception notes, and accessible reporting.
This is where last-mile operations can either strengthen or weaken accreditation readiness. A pharmacy may have strong internal documentation, but if delivery records are scattered, incomplete, or hard to retrieve, the audit trail breaks near the finish line.For more on the visibility layer, see Dropoff’s guide to last-mile delivery tracking.
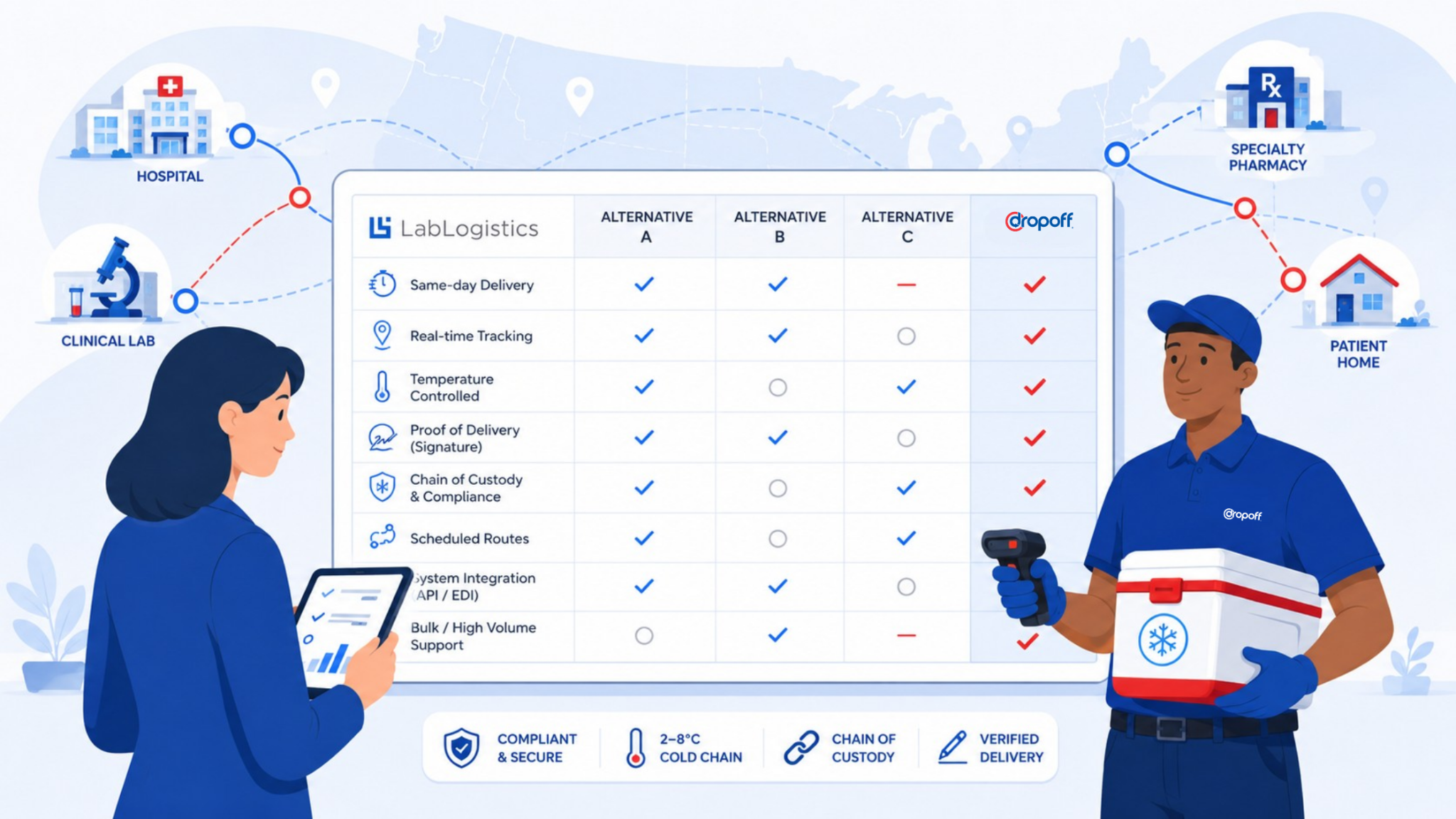
Specialty Pharmacy Courier Partner Checklist

A specialty pharmacy courier should be evaluated against more than speed, price, and coverage.
The better question is: can this courier produce the operating evidence our pharmacy may need later?
Use this checklist to evaluate whether a courier partner is aligned with accreditation-sensitive specialty pharmacy workflows.
1. BAA support when appropriate
The courier relationship should be reviewed for HIPAA implications. Depending on the courier’s role, access, and services, a BAA may or may not be required. The pharmacy should document that determination through its legal and compliance process.
2. PHI-aware workflows
Even when a courier is treated as a conduit, deliveries should be handled in a way that respects the sensitivity of patient information. That includes careful package handling, appropriate delivery notes, and avoidance of unnecessary patient information exposure.
3. Background-checked drivers
Specialty pharmacy deliveries should not depend on anonymous or loosely managed driver networks. Background-checked, vetted couriers support a more controlled delivery process, especially for healthcare and medication workflows.
4. Temperature-sensitive delivery capabilities
If the pharmacy handles temperature-sensitive medications, the courier should be able to support appropriate timing, handling, escalation, and exception procedures. The goal is not only to move the medication. The goal is to preserve the delivery conditions the pharmacy needs to defend.
5. Real-time tracking
Real-time tracking helps operations teams monitor delivery progress and intervene when something goes wrong. For specialty pharmacy workflows, ask what tracking shows in practice: courier location, pickup confirmation, delivery status, attempted delivery, delay alerts, return-to-pharmacy status, or exception notes.
Tracking should help the pharmacy act before a delivery problem becomes a patient access problem.
6. Time-stamped proof of delivery
Proof of delivery should be easy to retrieve and detailed enough to support internal review. At minimum, pharmacy teams should understand what delivery data is captured, where it is stored, who can access it, and how quickly it can be produced.
A strong proof-of-delivery record should answer: when was it delivered, where was it delivered, who received it when verification was required, and what happened if delivery failed?
7. Signature capture when required
Some deliveries require recipient verification or signature capture. The courier should support these workflows consistently and document them clearly.
8. Chain-of-custody documentation
For high-value, sensitive, controlled, or closely monitored medications, the courier should support handoff records that show who had custody and when.
9. Exception management
The courier should have clear protocols for failed attempts, patient unavailability, incorrect addresses, delays, temperature concerns, damaged packages, and returns.
The pharmacy should also know how exceptions are communicated and documented. A buried email, vague text, or late status update may not be enough.
Ask what happens after a failed first attempt. Who is notified? How quickly? Is the patient contacted? Is the pharmacy contacted? Is a reattempt scheduled? Is the package returned? Is the reason coded in a way the pharmacy can trend later?
10. Route, scheduled, same-day, and on-demand support
Specialty pharmacy delivery is not one workflow. Some deliveries are scheduled. Others are urgent. Some follow recurring routes. Others are patient-specific and time-sensitive.
A courier partner should be able to support the delivery model the pharmacy actually uses.
11. Reporting access for audits and quality reviews
Delivery data should be accessible for internal audits, accreditation preparation, payer inquiries, manufacturer reporting, and quality improvement.
12. Escalation support
When something goes wrong, the pharmacy should not be left decoding courier smoke signals. Escalation paths should be clear, timely, and documented.
Dropoff supports pharmacy delivery services and broader healthcare courier services with same-day and scheduled delivery, real-time tracking, digital confirmations, vetted couriers, customized logistics workflows, and 24/7 support. For more vendor evaluation criteria, see this guide to choosing a medical courier.
How to Prepare for Specialty Pharmacy Accreditation
The checklist should not live only in procurement. Compliance, operations, pharmacy leadership, and quality teams should all have visibility into courier performance when delivery affects patient access, medication integrity, or documentation.
A courier can look acceptable on cost and coverage while still creating accreditation friction if it cannot produce usable records when the pharmacy needs them.
Preparing for specialty pharmacy accreditation should not start with a binder. It should start with the actual workflow.
The goal is to understand how work happens, where documentation is created, where partner dependencies exist, and where the record could break under review.
Review the standards before building the workflow
Start by reviewing the relevant accreditation standards and mapping them to real operations.
This includes intake, patient management, clinical documentation, procurement, inventory, dispensing, distribution, quality review, complaint handling, performance improvement, and partner oversight.
Do not wait until the workflow is already baked into daily operations to discover that key documentation is missing.
Document how work happens
Accreditation readiness depends on evidence.
Pharmacies should document:
- Policies and procedures
- SOPs
- Staff training records
- Patient communication workflows
- Dispensing records
- Distribution records
- Delivery records
- Exception logs
- Complaint records
- Quality improvement activity
- Vendor review processes
FDB’s accreditation article points out that manual mapping of standards to documentation systems can create strain as organizations scale. That is a useful reminder: documentation should be built into daily workflows, not reconstructed after the fact.
Identify partner dependencies
Every partner that touches the patient experience, medication delivery, PHI, temperature-sensitive product, or documentation trail should be evaluated.
That may include technology vendors, call centers, courier partners, packaging providers, distribution partners, or other outsourced service providers.
For last-mile delivery, review:
- Who handles the package?
- What information does the courier receive?
- What delivery records are created?
- How are exceptions handled?
- How are failed deliveries escalated?
- How quickly can records be retrieved?
- Are courier issues reviewed in quality meetings?
Test record retrieval before survey season
Do not wait for a surveyor, payer, or manufacturer to ask for records.
Run a sample retrieval test:
- Pull a recent specialty medication delivery.
- Confirm the prescription and dispensing record.
- Confirm courier pickup.
- Confirm proof of delivery.
- Confirm recipient signature if required.
- Confirm temperature documentation if needed.
- Confirm exception notes if anything went wrong.
- Confirm who had custody at each point.
- Confirm the record can be retrieved quickly.
The goal is not to create a perfect record for one cherry-picked order. The goal is to see whether ordinary records are complete enough to stand up under review.
If the team has to manually reconstruct the delivery from dispatcher notes, patient calls, courier emails, and screenshots, the workflow is carrying hidden audit risk.
This kind of self-audit reveals gaps before they become formal findings.
Feed delivery data into quality improvement
Delivery issues should not sit outside the quality program if they affect patient access, medication integrity, or documentation completeness.
Useful delivery metrics may include:
- On-time delivery performance
- Failed delivery attempts
- Reattempt frequency
- Temperature-sensitive delivery exceptions
- Missing proof of delivery
- Patient unavailable trends
- Delivery-related complaints
- Return-to-pharmacy events
- Courier escalation response times
If a pharmacy uses service-level expectations with its courier, those expectations should be reviewed regularly. For related guidance, see Dropoff’s article on logistics SLA expectations.
Self-Audit: Is Your Courier Supporting Your Accreditation Posture?
Before your next accreditation review, evaluate whether your courier can support the same documentation, visibility, and control expectations your pharmacy is held to.
Start with practical questions:
– If a surveyor asked for delivery documentation tomorrow, could your team produce it quickly?
– Can your courier provide time-stamped proof of delivery?
– Are delivery exceptions documented in a way your compliance team can use?
– Can your team see when, where, and to whom a specialty medication was delivered?
– Are temperature-sensitive deliveries supported with appropriate workflows?
– Does your courier relationship align with your HIPAA and BAA review process?
– Are courier issues included in quality improvement conversations?
– Can delivery data be used for payer, manufacturer, or internal quality review?
A courier review is especially important if your team is seeing recurring failed attempts, incomplete proof of delivery, unclear exception notes, delayed escalation, temperature-sensitive delivery concerns, or manual record reconstruction before audits.
For specialty pharmacies, courier performance is not just a logistics concern. It is part of the operating evidence that supports patient access, documentation, and audit readiness.
Dropoff supports healthcare organizations with reliable same-day and scheduled delivery, real-time tracking, digital confirmations, vetted couriers, chain-of-custody support, healthcare delivery workflows, and 24/7 support. If your pharmacy is reviewing its delivery process as part of accreditation preparation, explore Dropoff’s pharmacy delivery services or connect with our team to evaluate your current courier workflow.
Specialty Pharmacy Accreditation FAQs
Specialty pharmacy accreditation is a formal review process that evaluates whether a specialty pharmacy meets recognized standards for patient management, medication handling, dispensing, distribution, documentation, quality management, and performance improvement. It helps pharmacies demonstrate that they can support complex specialty medication workflows safely and consistently.
Specialty pharmacy accreditation may not be universally required by law for every pharmacy. However, it is often required or strongly expected by payers, manufacturers, limited distribution drug programs, health systems, or network partners. In practice, accreditation can be important for market access, contracting, and operational credibility.
Specialty pharmacy accreditation requirements vary by accrediting body, but they commonly include patient management, drug procurement, inventory control, medication handling, dispensing, distribution, quality management, regulatory compliance, performance improvement, documentation, and partner oversight.
ACHC and URAC are both major accrediting bodies, but they have different emphases. ACHC’s pharmacy accreditation language includes strong operational and distribution-related language, including shipping methodology, records, communication, personnel training, organizational oversight, and quality improvement. URAC emphasizes care management, quality patient care, risk management, process improvement, and value to payers, manufacturers, and providers. Many pharmacies evaluate both based on payer, manufacturer, and operational requirements.
Timelines vary based on accreditor, readiness, documentation maturity, staffing, and operational complexity. URAC states that once an organization begins the process, it can be fully accredited in six months or less. Other accreditation paths may vary, especially if the pharmacy needs to close documentation gaps or redesign workflows before survey.
Costs vary by accreditor, organization size, scope, consulting support, and readiness work. The direct accreditation fee is only part of the total cost. Pharmacies may also need to invest in documentation cleanup, staff training, workflow updates, technology improvements, quality reporting, and partner or vendor review.
The accreditation belongs to the pharmacy, not the courier. But delivery partners can affect the pharmacy’s ability to document distribution, protect medication integrity, manage exceptions, support HIPAA-sensitive workflows, provide proof of delivery, and maintain audit-ready records. That is why courier evaluation should be part of accreditation preparation.
Specialty pharmacies should keep delivery records that show when the medication left the pharmacy, who handled it, where it was delivered, whether a signature or recipient verification was required, whether delivery was completed, and what happened if there was an exception. For temperature-sensitive medications, pharmacies should also document the workflow used to protect product integrity during delivery and escalation.
Proof of delivery helps document when and where a medication was delivered, who received it when signature is required, and whether any delivery exceptions occurred. For specialty pharmacies, proof of delivery can support patient communication, internal quality review, payer inquiries, manufacturer requirements, and accreditation readiness.
A specialty pharmacy should look for a courier partner with healthcare delivery experience, real-time tracking, time-stamped proof of delivery, signature capture, chain-of-custody support, temperature-sensitive delivery workflows, exception reporting, vetted couriers, reporting access, and BAA support when appropriate based on the courier’s role and PHI handling.
Some specialty medications are temperature-sensitive. The pharmacy needs workflows that protect product integrity through packaging, dispatch, delivery timing, handoff, exception management, and documentation.
The key issue is not only whether the medication was packed correctly. It is whether the pharmacy can show what happened if the delivery was delayed, missed, returned, or escalated. Cold chain delivery issues should be visible, documented, and reviewed as part of the pharmacy’s broader quality process.